| |
| |
| Kidney (Renal) Failure |
|
|
Normally, your kidneys perform their job flawlessly. But sometimes, the kidneys lose their ability to filter fluids and waste, causing dangerous levels of these substances to accumulate in your body. This condition is known as kidney (renal) failure and without treatment, the buildup of toxins, extra fluid and dangerous levels of minerals in your blood will eventually cause death. The following information addresses the most common questions about kidney failure and serves as a supplement to the discussion that you have with your urologist.
|
| |
|
What happens under normal conditions? |
|
|
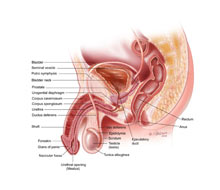
The kidneys are two bean-shaped organs, each about the size of your fist, located in the back of your upper abdomen on either side of your spine. When healthy, your kidneys cleanse the blood of waste products by producing urine. They also balance essential elements, such as sodium and potassium, while providing hormones necessary to regulate blood pressure and red blood cell production.
What is kidney failure?
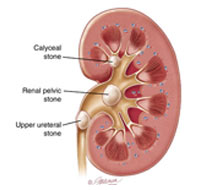
Kidney (renal) failure is a non-specific term for a decrease in the function of your kidneys. The diagnosis of kidney failure covers a wide spectrum of medical disease states. If at any point in the filtering process the kidney is blocked either because of direct kidney destruction (like diabetes) or by an indirect blockage (like having a kidney stone), the result can be kidney failure. |
| |
|
What are the different types of kidney failure? |
|
|
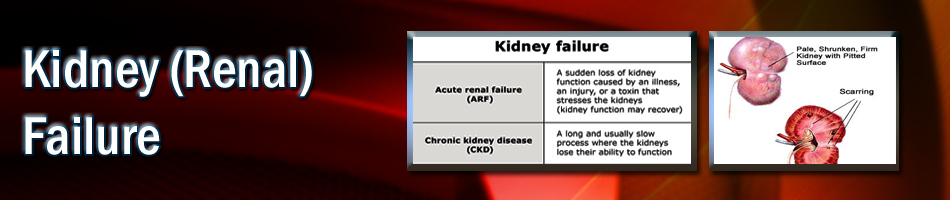
There are two main types of kidney failure – acute and chronic renal failure. Acute renal failure (ARF) occurs when the kidneys suddenly stop filtering waste products from the blood. Chronic renal failure (CRF) develops slowly with very few symptoms in its early stages.
What are the symptoms of kidney failure?
Symptoms vary depending on the severity of the kidney failure, its rate of progression and its underlying cause. The symptoms for ARF include fluid retention, internal bleeding, confusion, seizures and coma. A patient with CRF may not have any symptoms until normal kidney function declines to 20 percent or less. At that stage, an array of symptoms like the following may appear: abnormal urine tests, high blood pressure, unexplained weight loss, anemia, nausea, vomiting, metallic taste, loss of appetite, shortness of breath, chest pains, numbness and tingling, confusion, coma, seizures, easy bruising, itching, fatigue, headaches, decreased urine output, muscle twitches and cramps, bone weakening, bleeding in the intestinal tract, yellowish-brown skin color, unusual itching, excess fluid and sleep disorders. |
| |
|
How is kidney failure diagnosed? |
|
|
In order for a physician to diagnose kidney failure, the doctor must obtain laboratory results to confirm the suspicion. The most common blood test to use is a creatinine level test. Creatinine is a normal molecule found in your muscles. Your kidney, when functioning normal, should remove creatinine out of the blood and expel it. When the patient has some degree of kidney failure, it is common to have an increase in serum creatinine. This is often the first sign of kidney failure and it can occur even before a patient feels sick.
What are causes of kidney failure?
Acute renal failure (ARF): Is most likely to happen after complicated surgery or trauma, when blood vessels leading to kidneys become blocked, there are toxins in the system or urine flow is blocked. Fortunately with ARF, the function of the kidney can return to normal or near normal with proper treatment.
The causes of ARF can be classified as pre-renal, intra-renal or post-renal.
Pre-renal: The most common pre-renal causes of ARF include severe blood loss, dehydration, severe heart failure, excessive diuretic use and severe infection.
Intra-renal: Intrinsic renal failure can arise from disease of the small blood vessels, glomeruli, tubules or interstitium of the kidney. Some medication, like penicillin, can also cause renal failure.
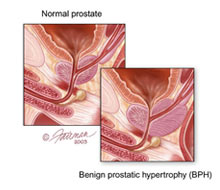
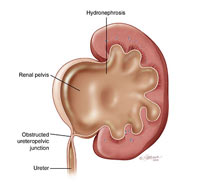
Post-renal: This type of ARF is caused by obstruction of urine flow beyond the kidneys. Most commonly this is seen in elderly men who cannot urinate properly because of an enlarged prostate, but any cause of blocked urine output is a risk factor. Obstruction can result in blockage of the ureters draining urine from the kidneys to the bladder, with bloating and stretching of the kidneys as a result (hydronephrosis – literally meaning "water in the kidney"). This ultimately progresses to destruction of the functioning kidney tissue if unrelieved.
Chronic renal failure (CRF): Is the consequence of a number of processes leading to permanent loss of kidney function. Its primary causes are high blood pressure and diabetes, but can also be due to urinary tract obstruction and kidney abnormalities, like polycystic kidney disease. |
| |
|
How is kidney failure treated? |
|
|
Acute renal failure (ARF): Most of the time, the kidneys will regain at least part of their function if the underlying cause is corrected. In some cases, ARF is so severe that dialysis with an artificial kidney machine is necessary. The dialysis can slowly be withdrawn as kidney function returns.
Treatment of pre-renal ARF is based on identifying and attempting to reverse the cause. Most patients will be expected to recover kidney function if they survive their underlying illness. Diuretics (mannitol, furosemide) may be helpful in the early stages of pre-renal ARF.
Chronic renal failure (CRF): Like ARF, the underlying disease needs to be treated. Hypertensive patients need to take their medications and diabetic patients need to control their blood sugars. Fortunately, kidneys have a large reserve of function. Even patients who have lost up to 80 percent of their kidney function do not need therapy since the small fraction of their kidneys that work is sufficient to clear the body of waste. For those patients whose CRF is so severe that they cannot survive on their residual kidney function, there are two options: dialysis and transplantation. Dialysis can be performed in one of two ways — either by hemodialysis (HD) or peritoneal dialysis (PD). HD requires that the patient be hooked to a dialysis machine at home or at a dialysis center, usually three times per week. Usually, the patient fills his/her abdomen with a solution through a tube that a surgeon implants in the abdomen. This washes the waste products away when the fluid is drained out of the abdomen.
When kidney function falls to below 10 percent of normal, conservative management is usually no longer adequate to control the symptoms of kidney failure. Dialysis is urgently needed when the patient has uncontrolled symptoms (e.g., nausea and anorexia), high blood potassium resistant to medical treatment, pericarditis (inflammation of the coverings of the heart) and nerve damage.
Kidney transplants have become the best treatment for many patients with end-stage kidney failure. Most centers have achieved very high success rates because of the development of more specific and less toxic immunosuppressant drugs over the last five to 10 years. Unfortunately, the success of transplantation has led to long waiting times for cadaveric organs and most patients remain on dialysis for years until an organ becomes available. There are now approximately 95,000 patients waiting for kidney transplants in the United States, but because of the organ shortage problems, only 13,000-16,000 patients receive kidney transplants per year. This has led to a special emphasis on live kidney donors. The advantage of having a live donor is the ability to perform the transplant with little waiting time, and in many cases, as a planned procedure before the recipient needs dialysis. Furthermore, the outcomes of a kidney transplant from a living donor are better than those with kidneys from deceased donors. At most large centers, living related donor and living unrelated donor kidney transplantations have become attractive options for patients to avoid the long waiting times for kidneys from deceased donors.
|
| |
|
| |
| Frequently asked questions: |
| |
My primary care doctor says that my large prostate has caused slight damage to my kidneys. What am I going to do? |
|
|
Untreated bladder obstruction caused by benign prostatic hyperplasia (BPH) can lead to chronic kidney failure. If BPH is the only reason you have CRF you will need to be evaluated for BPH treatment. Most of the time, you will have had other symptoms of BPH before developing kidney damage. A urologist can explain the various different options for treatment. |
| |
|
I have diabetes but my doctor says my kidneys are fine. Will I get kidney failure like my grandmother?
|
|
|
Recent studies have shown that careful control of your sugar levels can prevent all types of problems from diabetes including kidney failure. Regular checkups and lab work can help your doctor plan what medications can help your diabetes and your kidneys. |
| |
|
| |
I recently had acute kidney failure because of an antibiotic. Will my kidney function improve? |
|
|
If the only reason you had acute renal failure was because of the antibiotic reaction, your kidney function should return. Of course, you should never be given that antibiotic again. |
| |
|
I need a kidney transplant but I do not want to be on a list. Can my best friend donate his kidney? |
|
|
As long as your friend is healthy, has a compatible blood type and passes several blood and screening tests, he or she can. Living unrelated kidney operations are becoming common. Even strangers are coming forward to donate kidneys to patients in need of a kidney transplant.
|
| |
|
Can renal failure be caused by exposure to contrast dyes used in various X-ray tests? |
|
|
Acute renal failure occurs in up to 10 percent of patients exposed to some intravenous contrast materials (dye) used for X-ray tests. It is important to ask your doctor if you have any risk of kidney damage from X-ray tests that require the use of intravenous dye. The type of contrast material is extremely important. For example, the contrast material used for magnetic resonance imaging (MRI) test is not harmful to the kidneys. Preexisting kidney failure is an important risk factor
|
| |
|
| |
|
|